Hip labral tears in athletes: do you actually need surgery?
Maybe it started as a nagging ache after long runs or heavy squats. Maybe you noticed clicking or catching in the joint that you kept ignoring until it got bad enough to actually stop your training. You finally got imaging done and the report came back with the words you were not hoping to see: labral tear.
Now you are wondering if your athletic career just took a serious detour.
Here is what I want you to know before you spiral. A labral tear is not a death sentence for your training. And surgery is not automatically the next step. Let me break down what is actually going on, what the research says, and how athletes like you navigate this injury every day.
What Is a Hip Labral Tear?
The labrum is a ring of cartilage that lines the rim of your hip socket. Its job is to deepen the socket, improve joint stability, and act as a seal that keeps the femoral head centered. When it tears, that seal is disrupted.
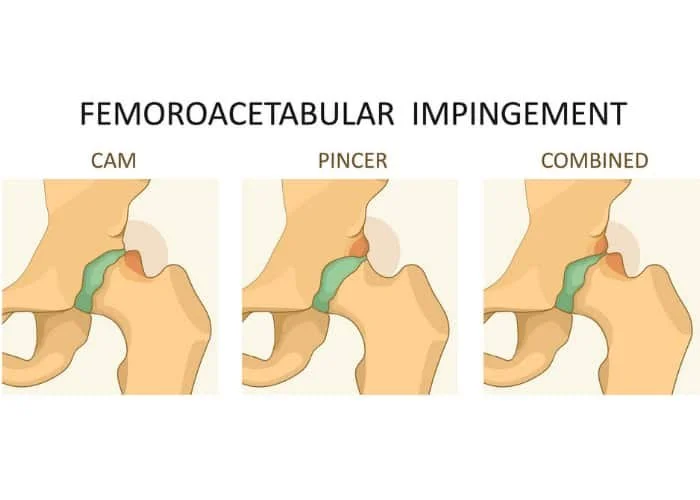
In athletes, labral tears are almost always associated with a condition called femoroacetabular impingement syndrome, or FAI. FAI happens when there is abnormal contact between the femoral head and the acetabulum during hip movement. There are two main types.
CAM morphology involves extra bone formation along the head-neck junction of the femur, creating an aspherical femoral head that pinches into the socket during hip flexion and internal rotation. This type is about three times more prevalent in athletes than the general population and is thought to develop as an adaptive response to repetitive high-load hip movement during growth, particularly in sports like football, hockey, soccer, and baseball.
Pincer morphology involves overcoverage of the femoral head by the acetabulum, essentially too much socket around the ball. This type accounts for the majority of FAI cases and is more common in women.
Many athletes have both.
What Does It Actually Feel Like?
The classic presentation is insidious. It usually does not start with one traumatic moment. It builds gradually as mild, episodic hip pain that gets worse with prolonged sitting, flares up when you stand from a chair, and shows up during training in positions of deep hip flexion or rotation.
Athletes often describe clicking, catching, locking, or a sense of stiffness in the joint. One of the most recognizable signs clinically is what is called the C sign, where someone cups their hand around the outside of their hip above the greater trochanter to describe where the pain lives.
Do You Actually Need Surgery?
This is the question everyone asks and the honest answer is: maybe, but probably not right away.
The current research is pretty clear that physical therapy should be the first line of treatment before surgery is even considered. Unfortunately, only about 44 percent of studies on FAI surgery even required patients to have tried conservative management first. That means a lot of athletes are going under the knife before exhausting options that could have resolved their symptoms.
Conservative management focused on hip and core strengthening in a supervised environment consistently produces better patient reported outcomes than generic home exercise programs. A solid non-operative plan addresses four things: postural alignment, core strength and endurance, hip muscle strength and motor control with an emphasis on the hip abductors, and lower body mobility. Manual therapy including hip joint mobilization and distraction techniques has also been shown to reduce pain and improve range of motion.
The honest timeline for conservative care is three to six months. If symptoms have not meaningfully improved in that window, surgery becomes a more appropriate conversation.

When Surgery Does/Does Not Makes Sense
A few examples of when surgery makes more sense than continuing with PT:
The athlete who has already done a legitimate three to six month course of supervised physical therapy, addressed their strength deficits, cleaned up their movement patterns, and is still symptomatic with significant functional limitations. Conservative care had its shot. Surgery becomes the appropriate next conversation.
The athlete with a large CAM morphology and a full thickness labral tear who is trying to return to a high demand rotational sport like baseball, softball, or hockey. The structural problem is significant enough that no amount of hip strengthening is going to eliminate the mechanical impingement happening at end range.
On the flip side, significant osteoarthritis, older age, prolonged symptom duration before treatment, and severe femoral anteversion greater than 25 degrees are all associated with worse surgical outcomes. Those athletes deserve an honest conversation about what surgery is realistically going to do for them before committing to it.
The bottom line is that surgery is not automatically right or wrong. It depends entirely on the individual, the structural findings, the symptom history, and what conservative management has or has not accomplished.
what about arthritis?
The question I get all the time is: "If I don't fix my labrum, am I going to get arthritis earlier?"
My honest answer? Maybe. But, here is the thing nobody tells you.
Yes, the labrum helps protect and distribute load across the joint. So losing that function over time could theoretically accelerate wear.
But, surgery in general is also trauma to the joint, and we know that carries its own risk of accelerating arthritic changes depending on the patient.
You are essentially weighing two unknowns against each other.
Until the research gives us a clearer answer, do not let the fear of arthritis be the deciding factor.
What This Means for You
A thorough evaluation that looks at how your hip is moving, where your strength deficits are, and what is actually driving your symptoms is often a better indicator of whether you need surgery than the MRI alone.
At Monarch Performance Physical Therapy, I work with athletes dealing with exactly this kind of injury every day. No guessing, no generic protocols. Just an honest assessment of what your body is actually doing and a plan built around your sport and your goals.
What I promise every athlete who walks through my door is transparency. If I do not think surgery is your next best step, I will tell you that. If I do not think PT alone is going to solve your problem, I will tell you that too. You deserve a straight answer, not a path of least resistance.
Book your initial evaluation today and let's figure out exactly what your hip needs!